 |
|||
|
|
|||
|
Page Title:
Health Card Physical Examination (Medical Screening) |
|
||
| ||||||||||
|
| 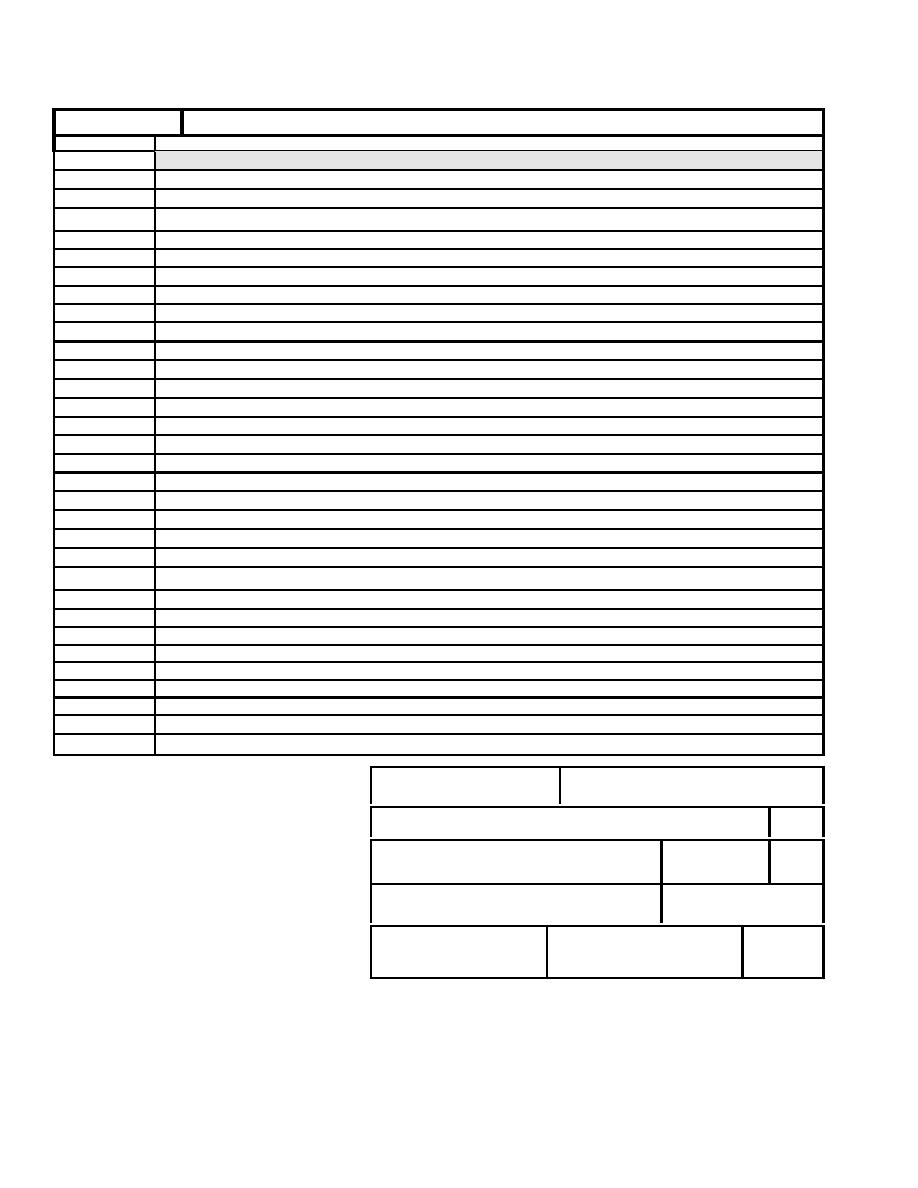 MANUAL OF NAVAL PREVENTIVE MEDICINE
HEALTH RECORD
DATE
SYMPTOMS, DIAGNOSIS, TREATMENT, TREATING ORGANIZATION (Sign each entry)
HEALTH CARD PHYSICAL EXAMINATION (MEDICAL SCREENING)
TODAY:
1. Are you suffering from any of the following:
a) Diarrhea?
YES
NO
b) Fever?
YES
NO
c) Vomiting?
YES
NO
d) Jaundice?
YES
NO
e) Sore throat with fever?
YES
NO
2. Lesions containing pus on the hand, wrist or an exposed body part?
(such as boils and infected wounds, however small)
PAST:
1. Have you ever been diagnosed as being ill with typhoid fever (Salmonella typhi), shigellosis (Shigella spp.),
Escherichia coli 0157:H7 infection (E. coli 0157:H7), or hepatitis A (hepatitis A virus)? YES
NO
If you have, what was the date of the diagnosis?
HIGH RISK CONDITIONS:
1. Have you been exposed to or suspected of causing a confirmed outbreak of typhoid fever, shigellosis,
E. coli 0157:H7 infection, or hepatitis A?
YES
NO
2. Do you live in the same household as a person diagnosed with typhoid fever, shigellosis, hepatitis A, or
illness due to E. coli 0157:H7?
YES
NO
3. Do you have a household member attending or working in a setting where there is a confirmed
outbreak of typhoid fever, shigellosis, E. coli 0157:H7 infection, or hepatits A?
YES
NO
4. Have you traveled outside the United States within the last 50 days?
YES
NO
Qualified
Not Qualified
EXAM COMMENTS:
____________________________
_______________________________
Patient Signature
Health Care Provider Signature
PATIENT'S IDENTIFICATION (USE THIS SPACE FOR MECHANICAL IMPRINT)
RECORDS MAINTAINED
AT
PATIENT'S NAME (Last, First, Middle initial)
SEX
RELATIONSHIP TO SPONSOR
STATUS
RANK/
GRADE
SPONSOR'S NAME
ORGANIZATION
DEPART./SERVICE
SSN/IDENTIFICATION NO.
DATE OF
BIRTH
CHRONOLOGICAL RECORD OF MEDICAL CARE
AUTOMATED STANDARD FORM 600 (Rev: 12/97)
154
|
|
Privacy Statement - Press Release - Copyright Information. - Contact Us |
